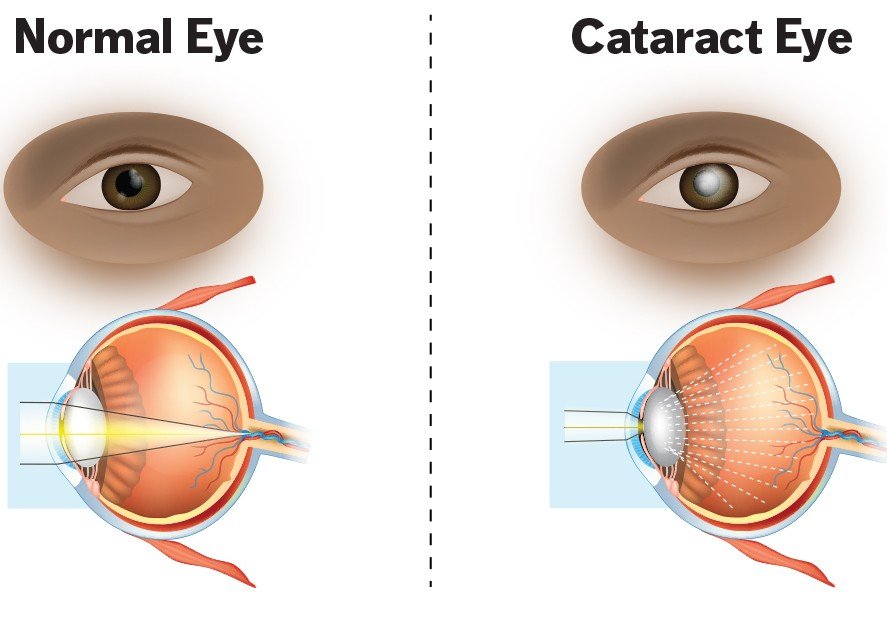
 SYMPTOMS OF CATARACTS
SYMPTOMS OF CATARACTS
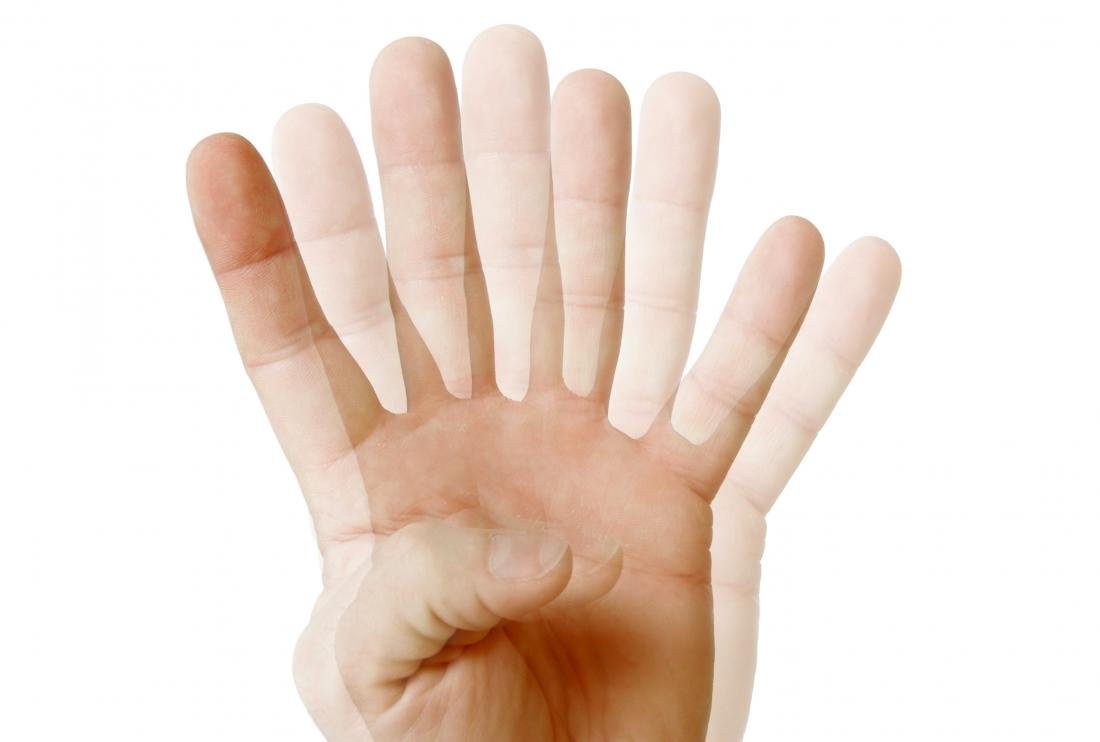
 Blurry vision Trouble seeing at night Seeing colors as faded Increased sensitivity to glare Halos surrounding lights Double vision in the affected eye. Aneed for frequent changes in prescription glasses
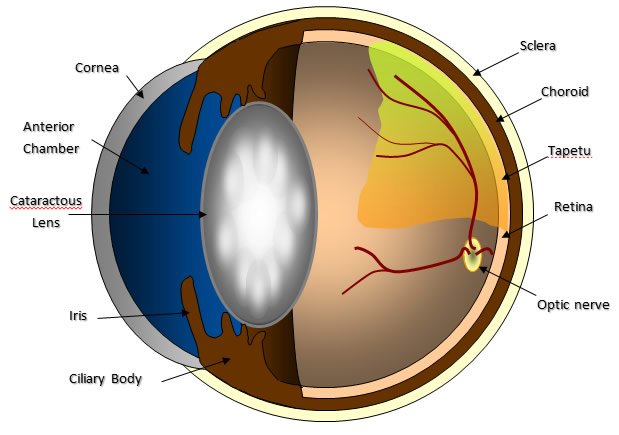
Blurry vision Trouble seeing at night Seeing colors as faded Increased sensitivity to glare Halos surrounding lights Double vision in the affected eye. Aneed for frequent changes in prescription glasses WHAT CAUSES CATARACTS ?
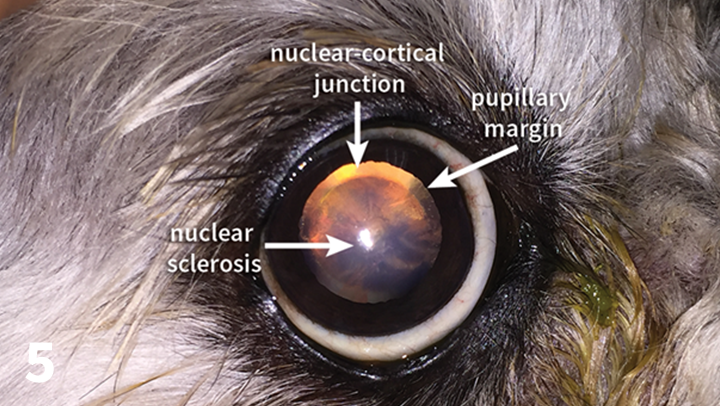
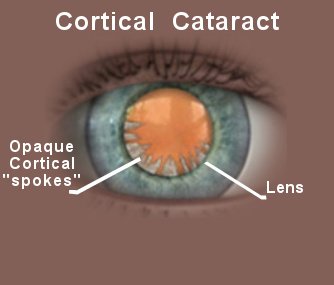
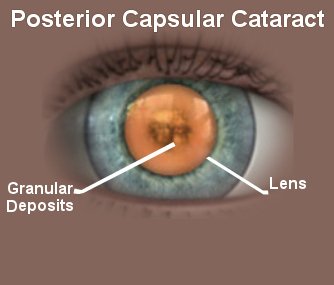
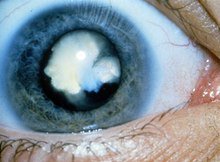
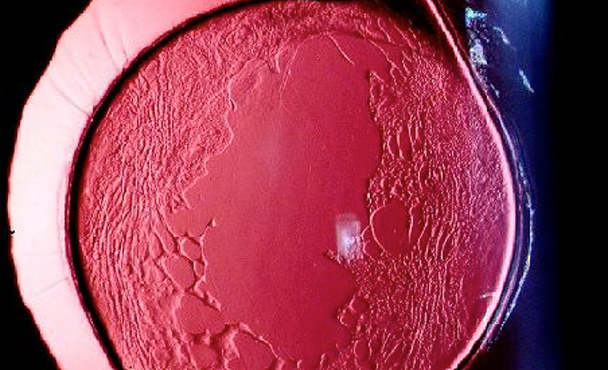
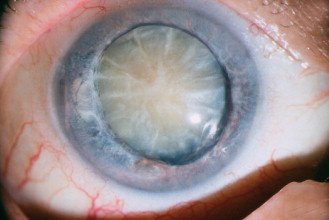
An overproduction of oxidants, which are oxygen molecules that have been chemically altered due to normal daily life Smoking Ultraviolet radiation The long-term use of steroids and other medications Certain diseases, such as diabetes Trauma Radiation therapy TYPES OF CATARACTS

RISK FACTORS OF CATARACTS










DIAGNOSING CATARACTS
TREATMENT

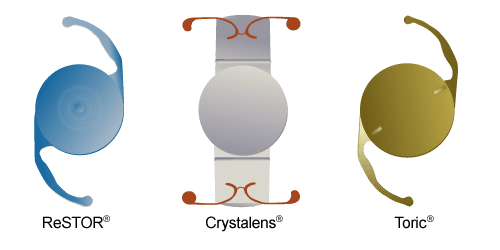
PREMIUM MONOFOCAL IOL (ASPHERIC IOLS)
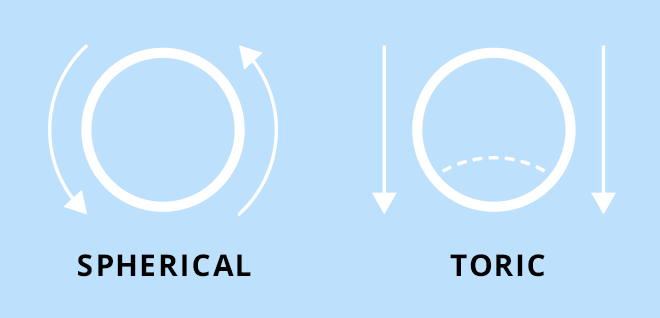
TORIC IOLS
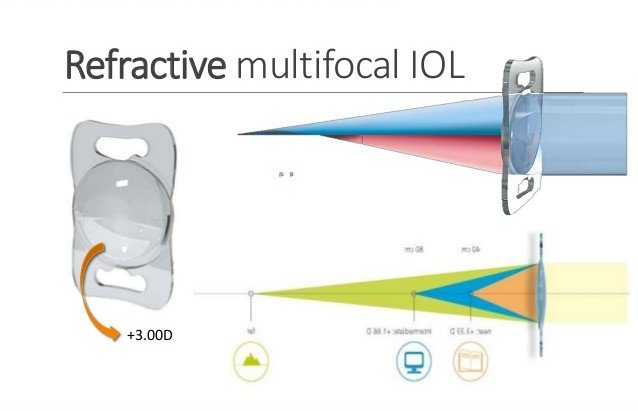
MULTIFOCAL IOLS
 WHICH PATIENTS ARE SUITABLE FOR THIS SURGERY?
WHICH PATIENTS ARE SUITABLE FOR THIS SURGERY?The most suitable patient is the one who strongly desires not to wear glasses after having eliminated medical contra-indications and exposed side eff ects especially halos.
Patients with significant night activity should be avoided as halos at night may disturb patients especially when driving.
These halos disappear for 20% of patients during the first month and for 40% of patients during the first year presumably by a Neuro-adaptation phenomenon.
They persist to varying degrees for the remaining 40% without significant reduction in activities.
 WHICH PREOPERATIVE ASSESSMENT?
WHICH PREOPERATIVE ASSESSMENT?An orthoptic assessment will be done to eliminate any microtropia. Analysis of the cornea must be scrupulous and any disease of the tear film must be treated beforehand because meibomian gland dysfunction can greatly disturb patients postoperatively.
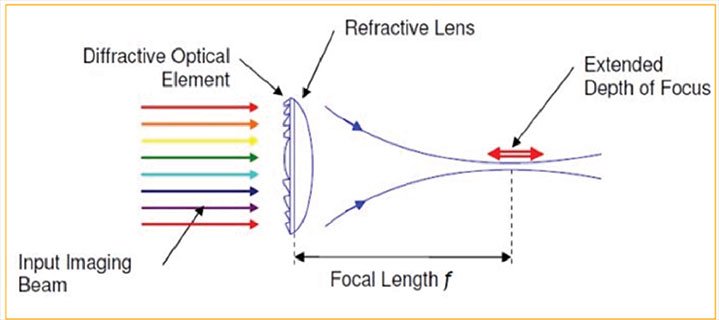
New apodized diffractive IOLs being pupil-dependent, photopic (Scheimpflug data) and mesopic (Colvard Pupillometer) measurement of the pupil will avoid narrow photopic or over dilated scotopic pupils.
Limits of 2mm in photopic and 5 mm in scotopic will avoid any pupillary refractive disorder postoperatively.
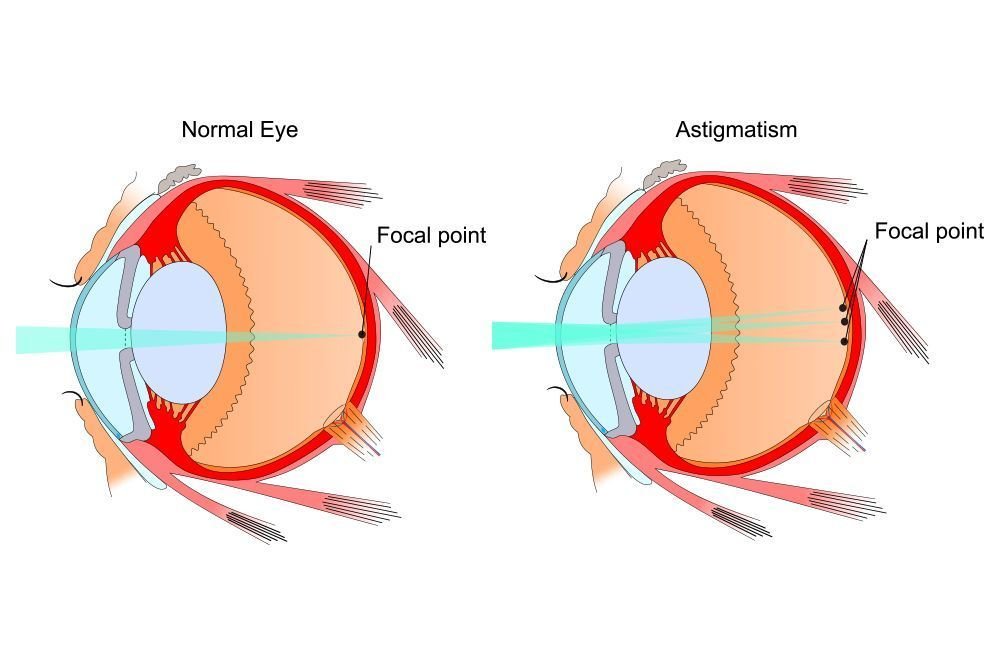
Astigmatism management is of paramount importance for obtaining ideal postoperative results with MFIOLs. A postoperative astigmatic error exceeding three-quarters of a diopter results in significant decline in visual quality.
A residual astigmatism lower than 0.50D does not seem to impair visual acuity, but we systematically treat astigmatism with toric lens if possible with the goal of no residual astigmatism.
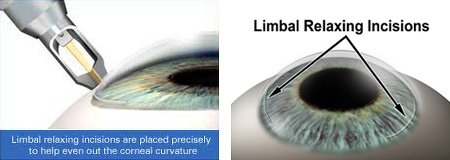
Corneal limbal incisions could be performing to treat lower astigmatism.
Pathological capsular bags or capsular bags at risk because of uncontrolled healing should be avoided in order to prevent any decentration of these IOLs.
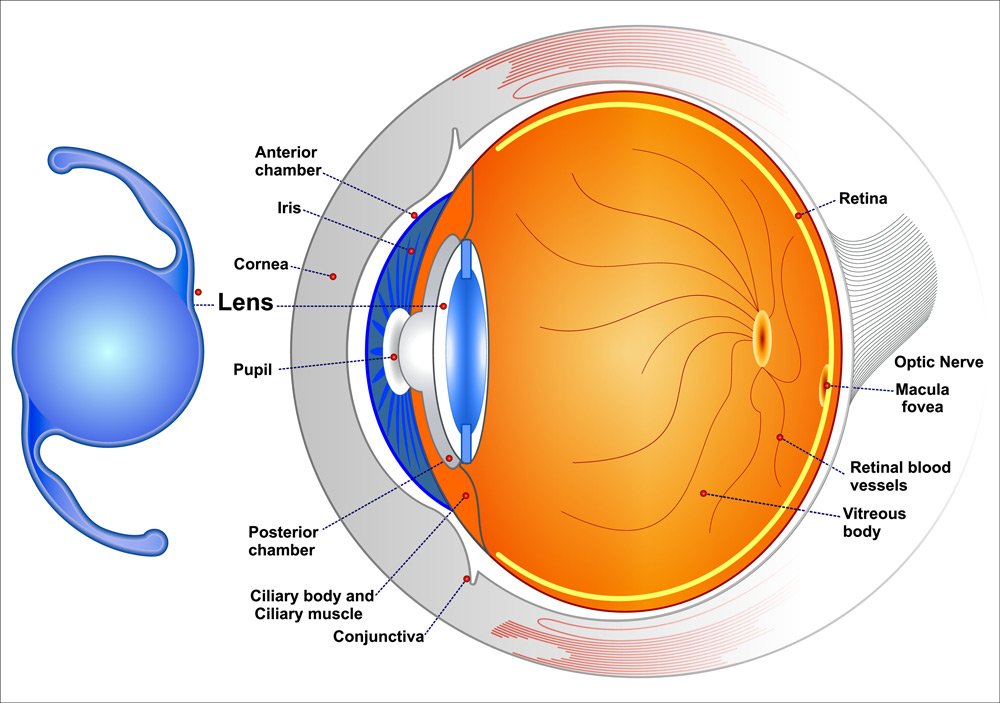
Finally a macular OCT analysis is performed when there is a doubt at fund us examination in order to eliminate an incipient macular traction syndrome or Epiretinal Membrane (ERM)
TYPES OF MULTIFOCAL INTRAOCULAR LENSES
WHICH SURGICAL TECHNIQUE?

OUTLOOK OF A CATARACT

PREVENTION OF CATARACTS
Protect your eyes from UVB rays by wearing sunglasses outside Have regular eye exams Stop smoking Eat fruits and vegetables that contain antioxidants Double vision in the affected eye. Keep diabetes and other medical conditions in check 7 SYMPTOMS OF CATARACTS







SEE YOUR DOCTOR
